New Considerations Since The Release of ATP III
Since the publication of ATP III in 2001, several major clinical trials of statin therapy have been published that looked at clinical end points. These trials addressed issues that may result in future reassessment of the ATP III treatment recommendations for selected patients.
Previously, cholesterol-lowering clinical trials in “high-risk patients” failed to conclusively confirm the relationship observed in epidemiologic studies in the lower ranges of LDL. In 2001, ATP III could not make recommendations on LDL-lowering therapy for persons with lower levels of serum LDL because there was no evidence at the time. The results of HPS (Heart Protection Study) helped to confirm the epidemiology studies with new clinical evidence at lower LDL levels.
A full review of the HPS (Heart Protection Study), PROSPER (Prospective Study of Pravastatin on the Elderly), ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial-Lipid Lowering Trial), ASCOT- LLA (Anglo-Scandinavian Cardiac Outcomes Trial – Lipid Lowering Arm), and PROVE IT (Pravastatin or Atorvastatin Evaluation and Infection – Thrombolysis in Myocardial Infarction 22) and their implications on the ATP III guidelines can be found in the library of this module.
Rationale for Recommended Low LDL Goal (<100) in High Risk Patients By ATP III
ATP III set the minimal goal in high risk patients to be <100 mg/dL. This level was as low as the clinical evidence supported in 2001. In addition, standard doses of statins used in secondary prevention trials achieved LDL <100 in a little more than half of high risk patients, with the remaining patients needing increased doses or a second agent added to the regimen.
Rationale for Optional Very Low LDL Goal (70 mg/dL) in High Risk Patients
In the HPS study, high risk patients – even those with a low baseline LDL <100 mg/dL had significant risk reduction when statins were introduced. HPS suggests that if you take high risk patients with a baseline of 100 mg/dL and reduce their LDL another 30%, you will achieve another 30% reduction in risk reduction. In the PROVE IT study high dose statin therapy reduced risks in 2 years as opposed to those using standard doses. PROVE IT and HPS results infer that the ATP III target for high risk patients of an LDL <100 mg/dL is not a sufficient goal and that more benefit can be achieved by further LDL lowering. In terms of absolute risk, it appears that 70 mg/dL is a preferred goal for very high risk patients.
So Did They Officially Lower The LDL Goal Recommendations?
No. The National Heart, Lung, and Blood Institute, the American Heart Association, and the American College of Cardiology Foundation found that four of these five post-ATP III studies had “implications” on the ATP III guidelines. Generally speaking, all clinical trial results in medicine must be replicated by other large clinical trials and performed in diverse populations before firm recommendation changes can be made. HPS and PROVE IT are not sufficient to make ATP III recommendation changes.
Furthermore, there have been concerns in what is known as the J- curve phenomenon. When a large population group has its blood cholesterol levels plotted on a graph against cardiovascular disease mortality, it usually results in a J-shaped curve. This curve shows that those with higher cholesterol levels are more likely to die from CVD. The curve also shows that those with very low cholesterol levels also have higher CVD mortality. This accounts for the J shape known as the J-curve phenomenon. It is thought that the group with the low cholesterol levels and higher mortality rate are different from the general population in ways that are not fully understood. There have been studies linking low serum cholesterol with cerebral hemorrhage, but a direct causal relationship between low LDL and increase morbidity and mortality has not be found. Reducing LDL to very low levels remains a concern.
Other questions remain in further lowering the LDL goals. In high risk patients with very high LDL baselines (>150 mg/dL), many will not be able to reach such low levels (<70 mg/dL) with any current LDL lowering drug regimen. A further consideration is whether more statin is necessarily safer? Studies have not found a significant increase in incidence of rhabdomyolysis or liver enzyme abnormalities at this time in high dose statins, but long term studies on risks remain to be done.
At this time, these recent clinical trials do not change the ATP III recommendations but offer a “therapeutic option” in selected high risk groups.
Implications for Clinical Management of LDL in High Risk Patients and Moderately High Risk Patients
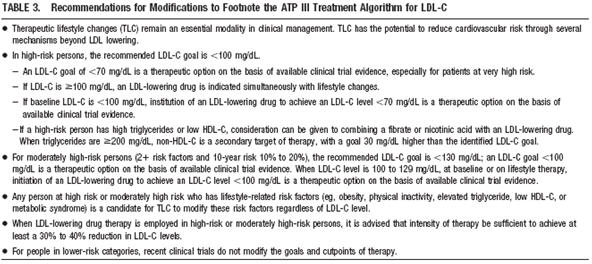
In high-risk persons, the recommended LDL-C goal is <100 mg/dL. When risk is very high, an LDL-C goal of <70 mg/dL is a therapeutic option on the basis of available clinical trial evidence. This therapeutic option extends also to patients at very high risk who already have a baseline LDL-C <100 mg/dL. Those in the category of very high risk: the presence of established CVD plus (1) multiple major risk factors (especially diabetes), (2) severe and poorly controlled risk factors (especially continued cigarette smoking), (3) multiple risk factors of the metabolic syndrome (especially high triglycerides ≥200 mg/dL plus non-HDL-C ≥130 mg/dL with low HDL-C [<40 mg/dL]), and (4) patients with acute coronary syndromes. When a high-risk patient has high triglycerides or low high-density lipoprotein cholesterol (HDL-C), consideration can be given to combining a fibrate or nicotinic acid with an LDL-lowering drug. For moderately high-risk persons (2+ risk factors and 10-year risk 10% to 20%), the recommended LDL-C goal is <130 mg/dL, but an LDL-C goal <100 mg/dL is a therapeutic option on the basis of recent trial evidence. The latter option extends also to moderately high-risk persons with a baseline LDL-C of 100 to 129 mg/dL. When LDL-lowering drug therapy is employed in high-risk or moderately high-risk persons, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels. Moreover, any person at high risk or moderately high risk who has lifestyle-related risk factors (e.g., obesity, physical inactivity, elevated triglycerides, low HDL-C, or metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level. The optional goal of <70 mg/dL does not apply to individuals who are not high risk. (Circulation. 2004;110:227-239.)
Summary of Implications of Recent Clinical Trials for ATP III Treatment Algorithm